
 |
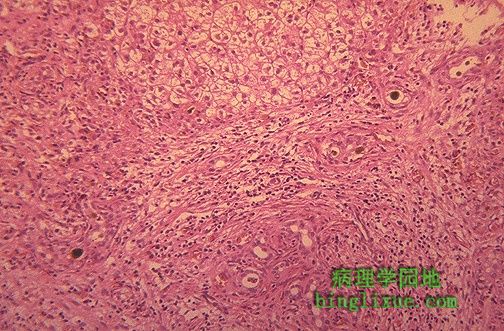
镜下见,肝外胆道闭锁导致肝脏大量黄绿色胆栓、假胆管增生(见于下面的中央)、广泛纤维化。如果有足够大的胆管可进行吻合并提供胆汁引流,该病即能够通过手术治愈。 Microscopically, extrahepatic biliary atresia leads to this appearance in the liver, with numerous brown-green bile plugs, bile duct proliferation (seen at lower center), and extensive fibrosis. If a large enough bile duct can be found to anastomose and provide bile drainage, then surgery can be curative. |
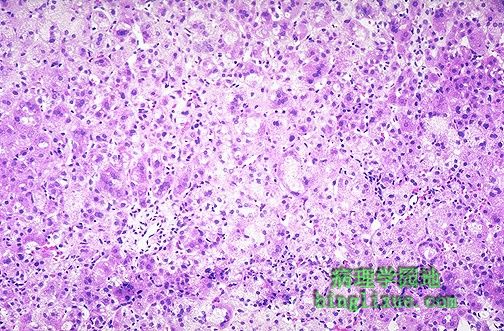 |
此图为胆道闭锁的主要不同诊断:这是一例新生儿巨细胞肝炎。图中可见具有病灶肝细胞坏死、巨细胞转化、淋巴细胞浸润、枯否细胞增生和胆汁淤积(此图未显示)的肝小叶紊乱。新生儿肝炎可为先天性或由病毒感染引起。许多新生儿在几个月内康复。 Seen here is the major differential diagnosis of biliary atresia: this is neonatal giant cell hepatitis. There is lobular disarray with focal hepatocyte necrosis, giant cell transformation, lymphocytic infiltration, Kupffer cell hyperplasia, and cholestasis (not seen here). Neonatal hepatitis may be idiopathic or of viral origin. Many neonates recover in a couple of months. |
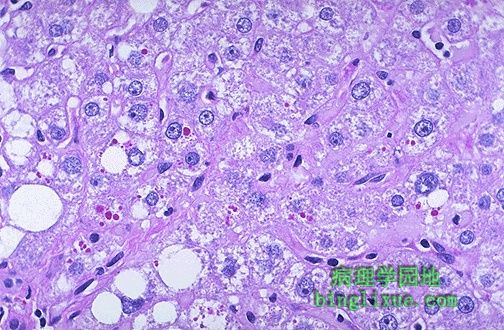 |
过碘酸-雪夫(PAS)染色时,门脉周围的红色玻璃样小球是α-1-抗胰蛋白酶缺乏症(pi-ZZ纯合子基因型患者)的特征表现。肝细胞未排泌的α-1-抗胰蛋白酶在肝内聚集,形成小球。它最终可导致大结节性肝硬化。这些患者还可能发生全小叶性肺气肿。 The periportal red hyaline globules seen here with periodic acid-Schiff (PAS) stain are characteristic for alpha-1-antitrypsin deficiency (a person with homozygous pi-ZZ genotype). The globules are intrahepatic collections of alpha-1-antitrypsin that is not being excreted from the hepatocytes. This may eventually lead to a macronodular cirrhosis. These patients are also prone to develop panlobular emphysema of lungs. |
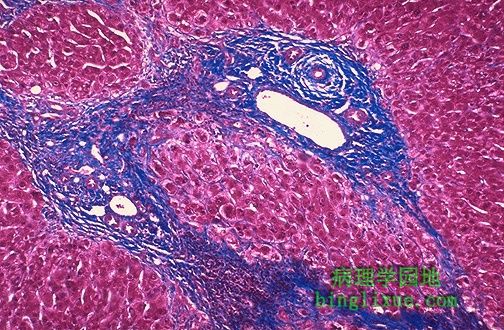 |
肝脏三色染色显示硬化性胆管炎时,广泛的门管区纤维化。肝细胞正常。 This trichrome stain of the liver demonstrates extensive portal tract fibrosis with sclerosing cholangitis. The hepatocytes are normal. |
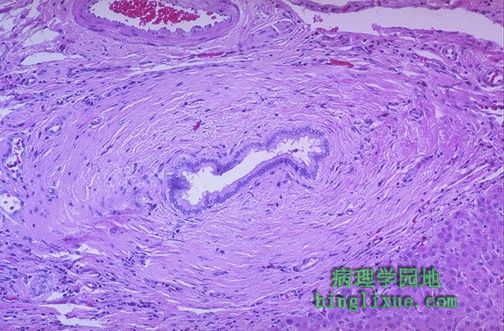 |
镜下可见,硬化性胆管炎患者的胆道周围环绕着明显的胶原结缔组织。 Microscopically, this bile duct in a case of sclerosing cholangitis is surrounded by marked collagenous connective tissue deposition. |